Chronic shoulder pain has a way of slowly reshaping daily life. What begins as mild discomfort when reaching overhead can gradually evolve into persistent pain that interferes with sleep, limits independence, and makes simple tasks like brushing your hair feel impossible.
For individuals living with severe shoulder arthritis, complex rotator cuff tears, or failed prior shoulder surgeries, mobility can steadily decline despite rest, medications, injections, and physical therapy. When conservative treatments no longer provide meaningful relief, advanced surgical solutions may be considered.
One of the most innovative options available today is reverse shoulder replacement, a procedure specifically designed to restore function in patients whose rotator cuff is too damaged for a traditional shoulder replacement to succeed.
At Philadelphia Hand to Shoulder Center, our physicians are nationally recognized for expertise in complex shoulder reconstruction and joint replacement procedures. With decades of specialized experience in upper extremity care, our team can help you determine whether reverse shoulder replacement is the right solution for restoring comfort, stability, and function.
What Is Reverse Shoulder Replacement?
To understand reverse shoulder replacement, it helps to first understand how a normal shoulder works. The shoulder is a ball-and-socket joint, where the ball (the head of the humerus) fits into a shallow socket (the glenoid). In a traditional shoulder replacement, the damaged ball is replaced with a metal ball, and the socket is resurfaced with a plastic component to maintain the joint’s natural structure.
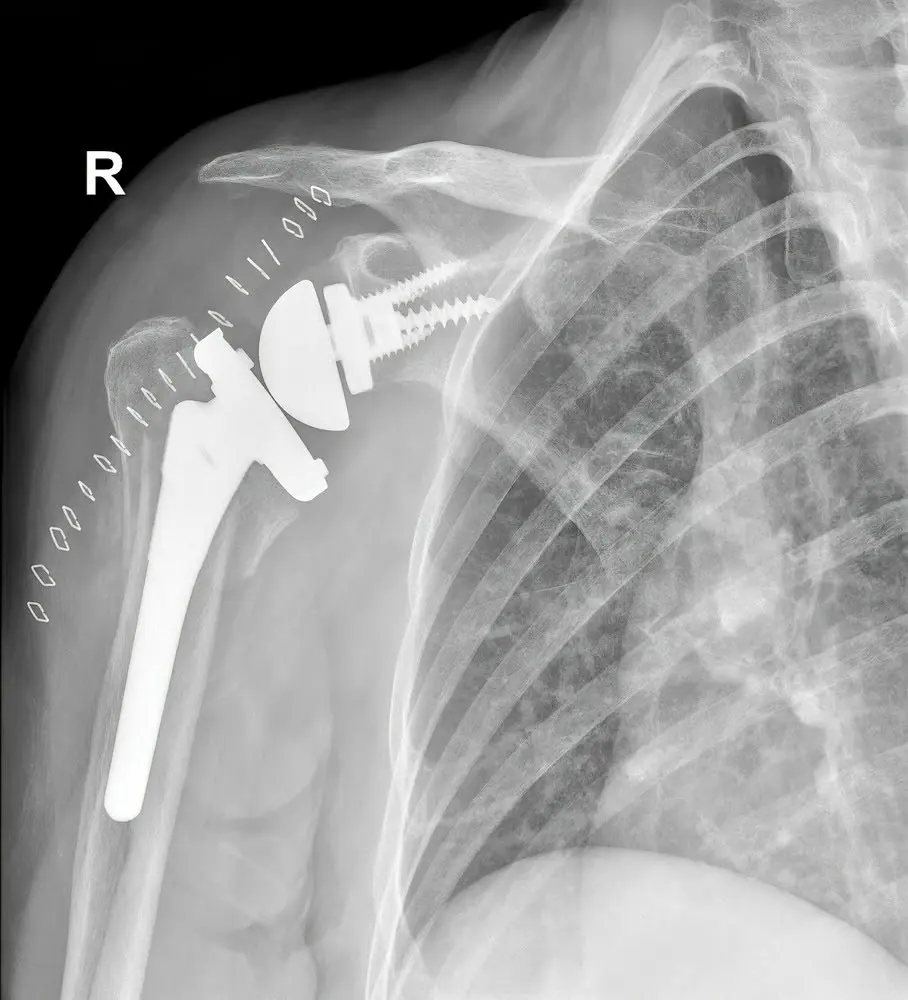
Reverse shoulder replacement, however, literally “reverses” the anatomy of the joint. The ball component is attached to the shoulder blade, and the socket component is attached to the upper arm bone.
Why reverse the mechanics?
In a healthy shoulder, the rotator cuff muscles help stabilize and move the joint. But when the rotator cuff is severely torn or nonfunctional, a traditional replacement may not restore stability or motion. By reversing the ball-and-socket configuration, the mechanics of the shoulder shift so that the deltoid muscle (a larger, stronger muscle) takes over much of the lifting function.
This innovative design allows patients with rotator cuff deficiency to regain improved shoulder elevation, stability, and pain relief, even when traditional surgery would not be effective.
Who Is a Candidate for Reverse Shoulder Replacement?
Reverse shoulder replacement is not necessary for every patient with shoulder pain. It is typically recommended for individuals with specific, complex conditions, including:
- Severe shoulder arthritis combined with rotator cuff deficiency (also known as cuff tear arthropathy)
- Massive, irreparable rotator cuff tears
- Complex shoulder fractures, especially in older adults
- Failed previous shoulder replacement surgeries
- Chronic shoulder instability not responsive to other treatments
Each patient’s condition is unique. At Philadelphia Hand to Shoulder Center, we conduct comprehensive evaluations that include a detailed medical history, physical examination, and advanced imaging studies, such as X-rays or MRI scans. This individualized approach ensures that surgery is recommended only when it is the most appropriate and beneficial option.
Age, activity level, bone quality, and overall health are also carefully considered before proceeding with reverse shoulder replacement.
How Reverse Shoulder Replacement Restores Function
For the right candidate, reverse shoulder replacement can provide significant improvements in both comfort and function.
Pain Relief
One of the most consistent benefits of reverse shoulder replacement is substantial pain reduction. By removing damaged bone surfaces and stabilizing the joint, inflammation and grinding are minimized, leading to improved comfort during both movement and rest.
Improved Mobility
Most patients regain the ability to lift their arm overhead — something that may have been impossible before surgery. Daily activities such as dressing, reaching into cabinets, and personal grooming often become easier and less painful.
Functional Strength
While reverse shoulder replacement is not designed to restore athletic-level strength, it can provide meaningful functional improvements. Patients can typically perform light household tasks and maintain independence.
It is important to set realistic expectations. While pain relief is often dramatic, full restoration of normal shoulder strength and range of motion is unlikely. The goal of this procedure is improved quality of life and functional independence — not necessarily a return to heavy lifting or high-impact sports.
Understanding the Limits of Reverse Shoulder Implants
Reverse shoulder replacement is highly effective, but it does come with limitations.
Activity Restrictions
Patients are typically advised to avoid:
- Heavy lifting (generally more than 20-25 pounds with the surgical arm)
- Repetitive overhead heavy labor
- High-impact sports
- Activities that place excessive strain on the joint
Range of Motion Expectations
While forward elevation often improves significantly, internal and external rotation may remain somewhat limited compared to a healthy shoulder.
Long-Term Protection
Protecting the implant is essential. Excessive strain, trauma, or noncompliance with rehabilitation guidelines may increase wear or risk of complications.
Our team at Philadelphia Hand to Shoulder Center provides clear guidance on safe activity levels and joint protection strategies to help maximize implant longevity.
Implant Longevity and Long-Term Outcomes
One of the most common questions patients ask is: How long will the implant last?
Modern reverse shoulder implants are designed for durability. Studies suggest that many implants last 10-15 years or longer, with continued improvements in materials and surgical techniques contributing to longer-term success.
Of course, you must note that there are several other factors that influence implant longevity, including:
- Patient age at the time of surgery
- Activity level
- Bone quality
- Adherence to rehabilitation guidelines
- Overall health
Younger, highly active patients may place greater stress on the implant, potentially shortening its lifespan. Older patients who follow recommended activity guidelines often experience durable outcomes for many years.
Ongoing follow-up appointments allow shoulder orthopedic specialists to monitor implant integrity and address any issues early. Advances in surgical precision, implant design, and post-operative care continue to improve long-term results.
The Recovery and Rehabilitation Process
Recovery from reverse shoulder replacement is gradual and structured.
Hospital Stay
Most patients stay in the hospital overnight or return home the same day, depending on overall health and surgical specifics.
Immobilization Period
A sling is typically worn for several weeks to protect the joint while initial healing occurs.
Physical Therapy
Rehabilitation begins with gentle range-of-motion exercises under professional supervision. Therapy gradually progresses to strengthening exercises as healing advances.
Timeline for Improvement
- First 6 weeks: Protection and gentle motion
- 6-12 weeks: Gradual strengthening
- 3-6 months: Continued functional improvement
- Up to 1 year: Ongoing gains in strength and mobility
Commitment to rehabilitation plays a critical role in maximizing surgical outcomes.
Consider This Life-Changing Solution
Reverse shoulder replacement reduces shoulder pain while also restoring independence, comfort, and confidence. For patients living with severe shoulder damage that limits daily life, this procedure can be transformative when performed by experienced specialists.
If you are dealing with persistent shoulder pain, limited mobility, or difficulty performing daily activities, we encourage you to schedule a consultation at Philadelphia Hand to Shoulder Center. Our team will provide a comprehensive evaluation and personalized treatment recommendations tailored to your goals and lifestyle.







Recent Comments